The use of low-dose CT scout or localizer images is proving suitable for MRI safety screening of patients with an unknown medical history, researchers from a top London facility have reported.
"The use of CT scouts is not specifically recommended in guidelines for MR safety screening, but the performance of CT scouts in this context has not been evaluated," Marco Borri, PhD, lead clinical scientist (MRI) and MR safety expert at King's College Hospital NHS Foundation Trust told AuntMinnieEurope.com. "We expected that they would be able to depict a number of implants, but it is important to assess their limits in the screening process, and to what extent they can be used for this purpose."
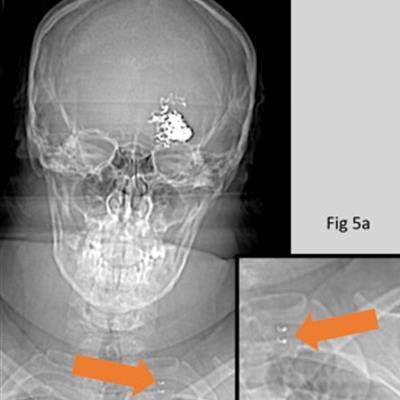
 (Left) CT scout image of patient with vagal nerve stimulator (VNS). (Right) patient with pacemaker. Both active implants were recognized as such, but the VNS was incorrectly identified as a pacemaker. The VNS (5a) can be distinguished from a pacemaker (5b) by the metallic attachments to the vagus nerve (orange arrow). Any active implant poses a high risk in MRI and would need to be investigated thoroughly before proceeding. All images courtesy of Hannah Barnsley, Sam Chigozie Uzoukwu, Marco Borri, PhD, and the ISMRM.
(Left) CT scout image of patient with vagal nerve stimulator (VNS). (Right) patient with pacemaker. Both active implants were recognized as such, but the VNS was incorrectly identified as a pacemaker. The VNS (5a) can be distinguished from a pacemaker (5b) by the metallic attachments to the vagus nerve (orange arrow). Any active implant poses a high risk in MRI and would need to be investigated thoroughly before proceeding. All images courtesy of Hannah Barnsley, Sam Chigozie Uzoukwu, Marco Borri, PhD, and the ISMRM.The ability to find and identify implants on radiological images is affected by both the quality of the image and the experience and skills of the reader, he explained. "In our study, the former was a limit only for a few implants -- those with both small size and fine mesh -- while the second affected a larger number of them. Both aspects should be optimized for effective screening."
The appeal of CT scouts
Increasing numbers of patients are presenting for MRI scans but cannot complete the safety questionnaires, the King's College group reported at the recent annual meeting of the International Society for Magnetic Resonance in Medicine (ISMRM) in London. CT scout images have low radiation dose and are faster and easier to acquire compared to plain film x-rays, which is still the recommended modality for MR safety screening for patients with unknown history.
In a study presented as a poster at ISMRM 2022, the researchers assessed the performance of CT scout images in detecting and identifying a range of head/neck and body implants. Using 40 head and neck and 40 body CT scouts, two readers reviewed the images for possible internal implants. 88% of implants were found and correctly identified, leading the authors to conclude that most visible implants are detectable.
"When screening patients who are not able to provide their own histories, or for whom such histories cannot be reliably obtained from others, and previous imaging is not available, plain film x-rays are recommended to identify implants. These should include the head/neck, chest, abdomen/pelvis, and the extremities if there are obvious post-traumatic changes," they noted.
However, acquiring plain film x-rays in multiple projections and positions can be difficult, especially for trauma or noncompliant patients, as it requires a significant amount of manual handling and potentially multiple operators. The quality of the images is also affected by operator experience, patient body habitus, and position, the study authors continued.
Key findings of London study
A subset of the 40 head/neck and 40 body CT scouts included one or multiple internal implants whose presence is not detectable by visually inspecting the patient. Two readers were shown the images in random order and asked to review them for possible implants. The readers -- one medical physicist (reader one) and one senior MRI radiographer (reader two) -- inspected the CT scouts on the PACS, and they were blind to any other patient details or image sets.
In 88% of cases, the readers found all implants (or their absence); and in 73% of cases, they correctly identified them. In 8% of cases, at least one implant was missed within an image containing multiple implants. Both readers scored similarly, with a slightly better performance in both finding and identifying implants from reader two, a clinical operator with more experience in reviewing CT images.
Both readers failed to identify two neurovascular stents, two coronary stents, and one of the three carotid stents (see figure below).
 (Left) CT scout image contains the missed carotid stent. (Right) Carotid stent correctly identified. The carotid stent in Fig. 3a, although visible, is partially obscured by superimposed anatomy. This case shows implants can be difficult to identify, and both image quality and the experience of staff can play a role.
(Left) CT scout image contains the missed carotid stent. (Right) Carotid stent correctly identified. The carotid stent in Fig. 3a, although visible, is partially obscured by superimposed anatomy. This case shows implants can be difficult to identify, and both image quality and the experience of staff can play a role.Both readers also missed a hidden frenum piercing, which was present within a projection with multiple implants. The small metallic foreign body was correctly identified, despite being superimposed over the dense bone of the skull base.
Additionally, reader one missed an iliac stent and a breast clip. But from the list of implants included in this work, all high-risk implants that have led to documented injuries or death following MRI, such as aneurysm clips and active implants, were identified. All active implants were recognized as such. But in some cases, they were incorrectly identified (e.g., pacemaker instead of VNS, as shown in the first figure).
Experience of readers
The two readers were chosen because they have different expertise and experience, but both are directly involved in decisions regarding patient safety in MRI, the authors told ISMRM 2022 attendees. While clinical experience in reviewing CT images was an advantage, they thought that both readers' results could be improved in some cases with training or further experience.
"The presence of two projections, both an anterior-posterior and lateral, helped to localize the position of an implant and to differentiate implants from internal pathology. This informs on the importance of multiple projections in any plain film modality," they explained. "However, some implants were not visible in the images. Both the neurovascular and coronary stents could not be detected as, despite being radiopaque, they are very small and had too fine a mesh to be depicted by this type of imaging."
Similarly, carotid stents or inferior vena cava (IVC) filters, which consist of fine metallic components, although visible, can be partially obscured by anatomy in a crowded projection. Furthermore, as in the case of the missed frenum piercing, rare or unexpected implants might be difficult to find, possibly regardless of the imaging modality, further highlighting the need for specific skills and training, according to the King's College team.
Within the selected set of implants, all those considered at high risk when exposed to MRI were found on CT scouts, even with often multiple distracting elements within the images. CT scouts are already being used as a screening tool for other purposes due to their ease of acquisition and low dose compared with x-rays, they said.
Overall, the study highlighted that in some cases they can be suitable for MR screening and that with sufficient training and dedicated experience, at least some of the missed implants could be detected.
Looking to the future
Future work planned in this area will compare CT scout performance to that of the recommended imaging modality, plain film x-rays, the authors noted. Furthermore, the dose of CT scouts should also be evaluated in comparison to the cumulative dose of a series of plain film x-rays.
"We are including more readers in our evaluation to better assess the impact of experience. We are also working towards providing the right set of skills to the clinical users involved in MR safety screening, and building training resources specifically to address this," Borri said.
"We think that the performance of CT scouts should be evaluated against the performance of the recommended modality, plain film X-ray. It is also worth investigating if CT scouts can be optimized for MR safety screening and what is the implication in terms of radiation dose. We are working towards addressing those questions as well," he concluded.


















