MRI is indispensable for evaluating football goalkeepers who present with suspected ligament and tendon injuries of the hand and wrist, and it contributes enormously to patient management, award-winning Brazilian researchers have reported ahead of this month's World Cup.
"Radiologists need to understand the anatomy and the full spectrum of fingers and thumb abnormalities and associated MRI findings," Dr. Tatiane Cantarelli, a musculoskeletal radiologist at HCor e Teleimagem and the Federal University of São Paulo (UNIFESP), and colleagues told attendees at the annual meeting of the International Skeletal Society (ISS), held in Barcelona, Spain, from 23 to 28 October.
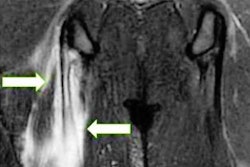
 Partial tear of the collateral ligament following trauma during football training in a 15-year-old male goalkeeper with left finger pain. (A) coronal and (B) axial T2-weighted fat-suppressed images show partial tear at the origin of the radial collateral ligament at the level of the proximal interphalangeal (PIP) joint of the fifth finger with diffuse ligament thickening (yellow arrows). There is bone contusion at middle phalanx (blue arrow) and PIP joint effusion (red asterisk). All figures courtesy of Dr. Tatiane Cantarelli and colleagues and presented at ISS 2022 in Barcelona.
Partial tear of the collateral ligament following trauma during football training in a 15-year-old male goalkeeper with left finger pain. (A) coronal and (B) axial T2-weighted fat-suppressed images show partial tear at the origin of the radial collateral ligament at the level of the proximal interphalangeal (PIP) joint of the fifth finger with diffuse ligament thickening (yellow arrows). There is bone contusion at middle phalanx (blue arrow) and PIP joint effusion (red asterisk). All figures courtesy of Dr. Tatiane Cantarelli and colleagues and presented at ISS 2022 in Barcelona."Hand injuries are usually traumatic," continued the authors, who received the best educational poster award from the ISS judges. "Lesions may occur from falls, axial loading of digits, or rotational force due to grasping activities. The proximal interphalangeal (PIP) joint of the fingers is the most injured joint in sports, followed by metacarpophalangeal (MCP) and carpometacarpal (CMC) joints of the thumb."
Clinical findings on MRI
MRI is the best modality for diagnosis and evaluation of soft-tissue trauma in the hand and wrist, particularly in the PIP and MCP joints, and it is useful for evaluating acute and chronic lesions of the stabilizing articular elements (volar plate and collateral ligaments) of the fingers and thumbs, including injuries to the pulley system, they stated.
"In my daily clinical practice, I see lots of soccer lesions as we work with the biggest teams in São Paulo," Cantarelli told AuntMinnieEurope.com. "Soccer is very popular in Brazil, and it's hard to find a Brazilian that doesn't like it."
Dislocations (dorsal, volar, or lateral) are common in ball-handling sports. Dorsal is the most common type, often involving hyperextension with axial loading. Volar plate injuries occur at the distal attachment with/without avulsion fracture of the base of the MCP joint.
Volar (straight volar, lateral volar, or rotatory) may involve force coupled with a volar thrust to the middle phalanx, and fractures/dislocations have a similar mechanism to dorsal dislocation. Volar plate injuries can be isolated or may occur in association with other injuries, such as collateral ligament tears, the researchers explained.
Distal injuries involve dorsiflexion and axial load stress, while intra-articular fractures include condylar fracture of the proximal phalanx (unicondylar, tibial bicondylar, or comminuted).
Injuries to the thumb
In the thumb, CMC joint injuries often are associated with fractures (e.g., Bennett's fracture). Dislocation without fracture is rare and involves rupture of the volar beak ligament with dorsal displacement of the first metacarpal, the authors noted.
Common injuries to the thumb MCP joint include dorsal dislocations (hyperextension with complete rupture of the volar plate, usually proximally), collateral ligament injuries, and skier's or gamekeeper's thumb (radially directed force on an abducted thumb), they continued.
 Thumb pulley injury. A 17-year-old male goalkeeper with pain after trauma on the thumb. (A, B) axial and (C) sagittal T2-weighted fat-suppressed images show thickening and irregularity of the A1 pulley (red arrow) and annular pulley or Av pulley (green arrow). Tenosynovitis of the flexor pollicis longus is visible (yellow arrow) with tendon integrity (orange chevron). Moderate diffused edema of the thenar muscles, surrounded with some fluid, related to the contusion (red asterisks), is also demonstrated.
Thumb pulley injury. A 17-year-old male goalkeeper with pain after trauma on the thumb. (A, B) axial and (C) sagittal T2-weighted fat-suppressed images show thickening and irregularity of the A1 pulley (red arrow) and annular pulley or Av pulley (green arrow). Tenosynovitis of the flexor pollicis longus is visible (yellow arrow) with tendon integrity (orange chevron). Moderate diffused edema of the thenar muscles, surrounded with some fluid, related to the contusion (red asterisks), is also demonstrated.MCP and CMC fractures tend to be stable due to the lower energy of sports-related injuries. Casting or splinting is recommended, with return to sport in between two and eight weeks. Malrotation or an unstable fracture requires closed reduction percutaneous pin fixation or open reduction internal fixation.
Most collateral ligament injuries are incomplete tears with minimal instability, and they are treated with taping or splinting. Return to sport may be immediate or in one to three weeks. Volar plate injuries require conservative management for closed stable volar plate injury with splinting. Inadequate treatment may lead to a "swan-neck deformity" (distal injury), and flexion contracture or pseudoboutonniere deformity (proximal injury) may develop, according to Cantarelli and her colleagues.
In thumb CMC joint injuries, closed reduction and assessment of stability with cast immobilization are necessary for four weeks. Instability may require percutaneous K-wire fixation, they added.
In thumb MCP joint injuries involving dislocation, simple immobilization for one to four weeks is recommended if the injury is stable. If it is not reducible (metacarpal head entrapped by the two heads of the flexor pollicis brevis, and interposition of the volar plate, collateral, or flexor pollicis longus), open reduction will be necessary.
If an avulsion fracture at the base of the proximal phalanx is present in a ligament injury, displacement of greater than 3 mm with rotation is the optimum repair, the authors wrote.
Use of ultrasound
For sports hand and wrist injuries, the radiologists at São Paulo generally use MRI as a first choice, because they can use the modality to access bone injuries, such as contusions, in addition to ligament or tendon injuries, especially for young athletes.
"Ultrasound is mainly used to follow up muscle injuries (e.g. assess healing, ossifications and size of the fluid collection) and to plan the return to play," Cantarelli said. "Another application for ultrasound in our institution is to assess whether the scar is causing muscle fiber movement restriction using dynamic maneuvers for chronic injuries."