VIENNA - With CT procedures on the rise and access to multislice scanners improving constantly, efforts to monitor and reduce patient radiation exposure are gaining momentum in tandem. New research presented at the 2009 European Congress of Radiology (ECR) examines whether reduced-energy CT and low-dose contrast media provide safer solutions without compromising pulmonary embolism (PE) image quality.
A Swedish study led by Dr. Mattias Kristiansson assessed the outcomes of reducing both the dose of iodine contrast and the kV output of a 16-detector-row CT scanner using a proprietary protocol (CareDose, Siemens Healthcare, Erlangen, Germany). His group tested 50 patients with a glomerular filtration rate less than 50 mL/min, as those with renal impairment are at particular risk of contrast-induced nephropathy (CIN).
Patients received 150 mL of iodine per 1 kg of body weight during a 12-second scan at 80 kV, effectively reducing the total volume of contrast medium compared with 16-slice MDCT "pulmonary standards" of 200 mL iodine per 1 kg during a 15-second 120-kV scan; this represented, Kristiansson said, a 25% relative reduction in iodine dose.
"To minimize scan time, we reduced scan area and used an automatic bolus tracking system with a 100-HU threshold with a four-second delay to the scan start," he noted. "We calculated mean density, image noise, and contrast-to-noise ratio [assuming 70 HU for a fresh blood clot] on 3-mm slices of the left main pulmonary artery and a lower lobe segmental artery."
None of the images generated using reduced-energy/low-dose parameters were considered nondiagnostic. Compared with a previous study (Humphries et al) that matched the CT protocol mentioned above, Kristiansson claimed "almost the same density in the pulmonary arteries, while the contrast-to-noise ratio remained almost unchanged."
"Most patients with increased risk of CIN can, in fact, be examined with 80-kV MDCT. If you optimize the contrast medium injection parameters, you will preserve diagnostic quality," Kristiansson said.
An ECR delegate asked whether these findings would hold true for patients with a high body mass index. This query was addressed in part by a subsequent presentation, in which Dr. Zsolt Szücs-Farkas, an attending radiologist at Bern University Hospital, Switzerland, discussed whether diagnostic quality was sufficient using pulmonary CT angiography at 80 kVp in patients weighing up to 100 kg (approximately 220 lb).
A cohort comprising 100 patients with suspected pulmonary embolism (no other exclusion criteria) underwent CT angiography (Somatom Sensation 16, Siemens Healthcare) at 80 kVp, using real-time automatic mAs-modulation (CareDose 4D) and a reference mAs of 150, following an injection of 75 mL contrast medium at 3 mL/sec. The patients were divided into six groups by weight.
The researchers measured noise and attenuation in the pulmonary arteries and calculated contrast-to-noise ratios. Three blinded radiologists independently analyzed overall image quality.
Szücs-Farkas concluded that "80 kVp gives sufficient diagnostic image quality at low exposure in patients weighing up to 100 kg."
There were no significant differences measured in image noise between patient groups above 50 kg and contrast-to-noise ratio in the 71-80 kg, 81-90 kg, and 91-100 kg groups. There also were no significant differences between all patient groups in the subjective ranking of enhancement, detectable ramification of the pulmonary arteries, subjective grading of noise in the vessels and mediastinum, or overall image quality.
 |
 |
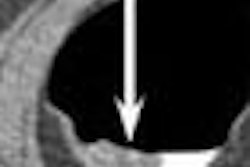
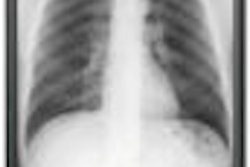
| All three CT images are from the same female patient weighing 95 kg with no pulmonary emboli. Above are two coronal maximum intensity projection (MIP) images, and below is a 1-mm thin transverse slice. At this body weight, 80-kVp CT angiography protocols provided good image quality and a high enough diagnostic confidence to exclude pulmonary embolism. All images courtesy of Dr. Zsolt Szücs-Farkas. |
 |
Discussing the study's limitations, Szücs-Farkas commented: "We clearly concentrated on diagnostic image quality and did not specifically evaluate the detection rate for pulmonary emboli. Also, we did not examine any patients with a body weight of more than 100 kg."
The mean attenuation of the pulmonary arteries exceeded 300 HU in all body weight groups.
Low-dose/high-concentration combination
A third study in this area concluded that a very low-dose/high-concentration iodine contrast protocol outperformed a high-dose/standard-concentration protocol in PE diagnosis. Researchers from Montpellier, France, and the University of Parma, Italy, compared the effects on attenuation and visualization of the pulmonary arteries.
A cohort of 143 patients with suspected acute PE was split into two groups. Group A received 16 g of high-concentration iodine contrast media before undergoing thoracic MDCT angiography. An AquilionOne 64-slice CT scanner (Toshiba Medical Systems, Otawara, Japan) at 120 kV was used to allow a short acquisition time (five to eight seconds).
Group B received 42 g of standard-concentration iodine before being scanned on the same machine, but with additional abdominal and pelvic evaluations. There were no significant differences between the patient groups. In all cases, the scan delay was determined using an automatic bolus tracking system.
Readers compared attenuation profiles of the two groups, looking at main, lobar, segmental, and subsegmental pulmonary arteries. Results showed a statistically significant difference (p = 0.03) between the groups.
"The low dose of high-concentration iodine significantly increased enhancement of pulmonary arteries, but also allowed us to significantly reduce the total amount of iodine injected," commented a researcher from Dr. Valentina Schembri's group.
On an additional note, they concluded, "this dose of iodine decreased iodine-induced risk."
By Rob Skelding
AuntMinnie.com contributing writer
March 9, 2009
Related Reading
320-detector-row CT cuts dose in triple rule-out exams, February 12, 2009
Dual-energy CT helps distinguish PE from other perfusion defects, December 2, 2008
MDCT for chest pain: Whom to scan, when to discharge, August 22, 2008
Multislice CT plus D-dimer testing sufficient for excluding pulmonary embolism, April 21, 2008
Low-dose CT yields equivalent value for PE in pregnancy, November 27, 2007
Copyright © 2009 AuntMinnie.com